
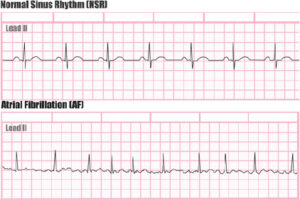
What is Atrial Fibrillation (AF)?
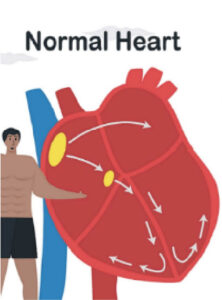
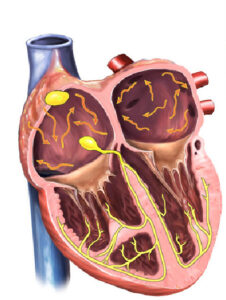
The heart consists of four chambers: two upper chambers, the right and left atria, and two lower chambers, the right and left ventricles. These chambers normally contract in a regular alternating pattern. However, in atrial fibrillation, the two upper chambers (the atria) quiver in a rapid and irregular pattern. This often results in an elevated and irregular heartbeat. Atrial fibrillation is the most common arrhythmia in the United States with over 12 million people (about twice the population of Arizona) expected to experience it by 2030.
Abbott. What is Atrial Fibrillation (Afib)?
https://www.structuralheart.abbott/patients/stroke-risk-reduction/atrial-fibrillation-laa
In the early stages of atrial fibrillation, episodes tend to be intermittent; this is called paroxysmal atrial fibrillation. During this stage, patient’s heart can correct atrial fibrillation back to normal rhythm spontaneously, usually within a few days.
Atrial fibrillation tends to be a progressive disease, and if left alone, over 70% of the time it will move on to more advanced stages. In persistent atrial fibrillation state, patient remains in atrial fibrillation continuously, and requires an intervention such as a cardioversion or using antiarrhythmic medications to restore normal rhythm. If one remains in persistent atrial fibrillation for prolonged periods and interventions are ineffective, the patient is considered to be in permanent atrial fibrillation.
Northwestern Medicine. Atrial Fibrillation
Atrial fibrillation may behave randomly, and it may be impossible to predict when these episodes will occur, how long it will last, or what the rate of progression will be. This makes it more frustrating for patients as well as challenging to manage for physicians.
What causes Atrial Fibrillation?
The exact cause of atrial fibrillation is not always known. However, certain conditions canincrease the risk of developing AF. These include hypertension, diabetes, coronary artery disease, heart valve problems, and sleep apnea. Older age and a family history of AF also raise the risk.
Lifestyle factors and specific triggers can also play a role. While modifying these factors won’t eliminate the risk of AF, studies show that reducing exposure to certain triggers can significantly
lower the incidence. These triggers include:
- Alcohol
- Caffeine
- Sleep disturbance
- Dehydration
- Stimulants (e.g., decongestant)
- Sleep apnea
- Major illness
- Major surgery
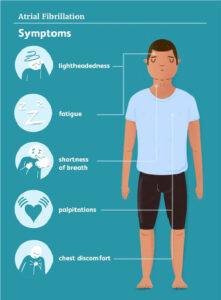
What are the symptoms of Atrial Fibrillation?
- Palpitations, often irregular and rapid
- Fatigue
- Shortness of breath
- Reduction in exercise tolerance
- Dizziness
- Chest discomfort
Surprisingly, a significant percentage of patients with atrial fibrillation do not experience any symptoms, even when their heart is beating rapidly and irregularly.
Is Atrial Fibrillation dangerous?
Atrial fibrillation (AF) is not considered a life-threatening rhythm problem. However, if untreated, it can lead to three major health problems:
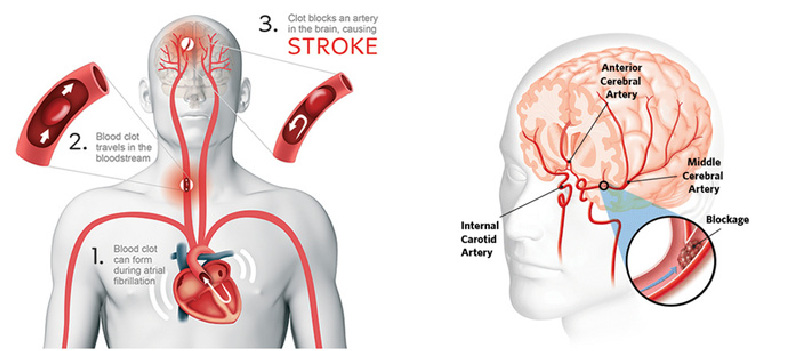
- Increased risk of stroke
If the top chambers of the heart, the right and left atria, are quivering and not contracting regularly, blood does not pump properly through these chambers which can lead to the formation of blood clots. A blood clot may dislodge and travel to the brain which can result in a stroke.
Arizona Heart Arrhythmia Association. Atrial Fibrillation Ablation https://www.azheartarrhythmia.com/contents/ep-procedures/atrial-fibrillation-ablation
- Increased risk of cardiomyopathy (weakening of heart muscle)
Atrial fibrillation often leads to elevated heart rate. If sustained, this elevated heart rate can place excessive stress on the heart muscle, weakening it over time leading to congestive heart failure, which can be serious. - Significant reduction in Quality of Life
Because atrial fibrillation can lead to inefficiency of heart function, patients may develop various symptoms. In many cases, these symptoms can be debilitating, significantly reducing the patient’s quality of life
However, when these issues are adequately addressed, patients with atrial fibrillation often lead a normal life expectancy with good quality of life.
How do I know if I have Atrial Fbrillation?
This varies by case. Some patients develop the symptoms mentioned above, which lead to a diagnosis of atrial fibrillation. Others may have no symptoms and are diagnosed with atrial fibrillation incidentally during a routine physical examination or preoperative ECG evaluation. Additionally, some patients may get a notification from a device such as a smartwatch, Kardia, blood pressure machine indicating an irregular rhythm.
What tests are needed to diagnose Atrial Fibrillation?
- ECG/EKG: This is typically performed in a doctor’s office, urgent care, emergency department, or hospital setting. Small electrodes (stickers) are placed on your chest, arms, and legs, then a 12-lead ECG/EKG is recorded.
Johnson&Johnson. 5 Things We Now Know About Atrial Fibrillation. https://www.jnj.com/innovation/5-things-we-now-know-about-atrial-fibrillation
- 2–4-week monitor: A small patch about the size of your palm is placed on your chest for 2-4 weeks to record rhythm continuously. You can take a shower, and carry on most activities while wearing this monitor, although swimming should be avoided

Diagnostic and Interventional Cardiology (DAIC). Zio by iRhythm Shows Significantly Higher Documentation of Atrial Fibrillation and Atrial Flutter Compared to Holter Monitors, Event Monitors. https://www.dicardiology.com/content/zio-irhythm-shows-significantly-higher-documentation-atrial-fibrillation-and-atrial-flutter
- Implantable loop recorder: This device is the size of a paper clip and can be inserted under the skin on the left side of your chest to continuously monitor rhythm for up to 3-4 years and report any atrial fibrillation to your physician automatically. It has Bluetooth technology built in and with an app on your phone, it can relay all downloaded data to the central surveillance center.

Medtronic. Cryptogenic Stroke Overview Brochure. https://www.medtronic.com/content/dam/medtronic-wide/public/united-states/medical-specialties/electrophysiology/cryptogenic-stroke-overview-brochure-en.pdf
- Apple Watch / Kardia / Fitbit / Android smartwatch: These devices, equipped with ECG recording capabilities can help document atrial fibrillation. Patients can initiate an ECG recording anytime they develop symptoms. Typically, these devices record for 30 seconds and will interpret the rhythm as either normal (sinus) or possible atrial fibrillation.

Apple. ECG App and Irregular Heart Rhythm Notification Available Today on Apple Watch. https://www.apple.com/newsroom/2018/12/ecg-app-and-irregular-heart-rhythm-notification-available-today-on-apple-watch/
How is Atrial Fibrillation treated?
There are three crucial issues to address in treating atrial fibrillation:
- Reducing risk of stroke.
- Reducing the stress to your heart.
- Improving your quality of life.
1. Reducing the Risk of Stroke
The primary concern for all atrial fibrillation patients is the increased risk of stroke. The risk of stroke is often assessed by a CHA2DS2-VASc Score which calculates the patient’s risk based on factors such as age, sex, hypertension, diabetes, prior stroke, prior heart attack, etc.For patients at moderate to high risk for stroke, blood thinning medications (anticoagulants) are usually recommended unless there is a significant contraindication such as major bleeding risk or high risk of falls.Unlike older blood thinners (e.g. warfarin/Coumadin), newer anticoagulants known as DOACs, (direct oral anticoagulants) such as apixaban (Eliquis) and rivaroxaban are much easier to use. The have fewer interactions with other medications, and do not require dietary restrictions or frequent blood tests. They are safer because they are absorbed and broken down by the body in a very predictable way. These medications have been shown in large clinical trials to significantly reduce the risk of stroke.Because these are potent blood thinners, it is important to avoid activities that increase the risk of injury or falls. Activities such as riding bicycles or motorcycles, engaging in contact sports, downhill skiing, climbing ladders, or using power tools should be avoided. For some patients, using a walking stick, cane, or walker may help improve balance and reduce the risk of falls.You should also avoid other blood thinning medications such as aspirin, ibuprofen, or other non-steroidal anti-inflammatory medications unless specifically approved by your physician.
It is advisable to wear a medical ID bracelet or necklace to identify that you are taking a blood thinning medication. Most emergency departments carry a reversing agent for blood thinners, and it is particularly important for emergency personnel to know that you are on a blood thinning medication in case of serious injury or bleeding.

You should inform your doctor if you experience recent falls, balance or gait issues, or if you have history of major bleeding problems (especially requiring a blood transfusions). You should also let your doctor know if you observe blood in your urine or stool or notice that your stool turns black and tarry.
If you get a superficial cut while on a blood thinner, applying prolonged pressure usually stops the bleeding. However, if you sustain a deeper cut or head injury, you should seek medical attention immediately, even if you feel fine. Before any medical procedure, dental work, or surgery, you must inform your healthcare provider that you are taking a blood thinner.
2. Reducing stress to your heart
When in atrial fibrillation, your heart rate is often much higher than normal, typically above 100 beats per minute even at rest. A constant elevated heart rate can cause stress to the heart and eventually may lead to weakening of the heart function, thus resulting in heart failure. Therefore, controlling the heart rate when you are in atrial fibrillation is important. There are several medications that can slow the heart rate during AF.
3. Improving quality of life
Atrial fibrillation can cause a wide range of symptoms such as palpitations or heart racing, fatigue, shortness of breath, dizziness/lightheadedness, reduced exercise tolerance and chest pain. As a result, atrial fibrillation may significantly limit you at work as well as other activities and hobbies. There are medications and/or procedures that can improve your quality of life by minimizing symptoms associated with atrial fibrillation. These approaches will be discussed later.
How do I know if I am at an increased risk of stroke? Do I need an anticoagulant (blood thinner)?
How do I know if I am at an increased risk of stroke? Do I need an anticoagulant (blood thinner)?
The primary critical issue to address in all atrial fibrillation patients is the risk of stroke. The risk of stroke for each atrial fibrillation patient is often assessed by a CHA2DS2-VASc Score which calculates the patient’s risk based on risk factors such as age, sex, hypertension, diabetes, prior stroke, prior heart attack, etc.
CHA2DS2-VASc
| Condition | Points | |
|---|---|---|
| C | Congestive heart failure (or Left ventricular systolic dysfunction) | 1 |
| H | Hypertension: blood pressure consistently above 140/90 mmHg (or treated hypertension on medication) | 1 |
| A2 | Age ≥ 75 years | 2 |
| D | Diabetes Mellitus | 1 |
| S2 | Prior Stroke or TIA or thromboembolism | 2 |
| V | Vascular disease (e.g. peripheral artery disease, myocardial infarction, aortic plaque) | 1 |
| A | Age 65–74 years | 1 |
| Sc | Sex category (i.e. female sex) | 1 |
Low risk: male 0; female 1
Low-moderate risk: male 1; female 2
Moderate-high risk: male ≥ 2; female ≥ 3
If a patient is at a moderate to high risk for stroke, blood thinning medication (anticoagulant) is usually recommended unless there is an absolute contraindication due to major bleeding risk or fall risk. Even in low/moderate risk patients, there will be certain situations where anticoagulation is recommended, e.g. anticipation of a cardioversion or an ablation procedure. This should be further discussed with your physician.
Can Atrial Fibrillation Be Treated with medications?
There are two distinct categories of medications in treating atrial fibrillation: rate-controlling medications and rhythm-controlling medications (antiarrhythmic medications).
1. Rate Controlling Medications
When in atrial fibrillation, your heart rate will tend to increase significantly, often well above 100 beats per minute at rest. This elevated heart rate is a major cause of uncomfortable symptoms associated with atrial fibrillation. Therefore, the purpose of these medications is to slow down your heart rate to reduce the severity of your symptoms and to lessen the stress on your heart.
These medications do not prevent or stop atrial fibrillation. Therefore, the frequency or duration of your atrial fibrillation episodes will not improve with these medications.
There are two main categories of rate-controlling medications:
A. Beta-blockers
1. Metoprolol succinate (Toprol), metoprolol tartrate (Lopressor), atenolol (Tenormin)
2. Beta-blockers slow your heart rate and lower your blood pressure (often used as blood pressure controlling agent).
3. Potential side-effects can be fatigue, shortness of breath (especially if you have history of lung problems such as asthma or COPD (Chronic Obstructive Pulmonary Disease)), dizziness/lightheadedness, especially if it slows down your heart rate or lowers your blood pressure too much. At higher doses, some may experience weight gain, erectile dysfunction, and depression.
B. Calcium channel blockers
1. Diltiazem (Cardizem), verapamil (Calan)
2. Calcium channel blockers also lower your blood pressure (often used as blood
pressure controlling agent).
3. Potential side-effects include ankle/feet swelling, constipation,
dizziness/lightheadedness, especially if your blood pressure gets too low.
C. Digoxin
1. This is an old drug that is rarely used as a primary agent to slow down heart rate in atrial fibrillation.
2. It is mostly used when a patient’s blood pressure is too low to use beta blockers or calcium channel blockers since, unlike those drugs, digoxin does not have an effect on blood pressure.
3. This medication requires close blood level monitoring (blood tests).
2. Rhythm-controlling medications (antiarrhythmic medications)
There are two important things you need to know about a rhythm controlling medication (Antiarrhythmic medication) approach:
• The goal of a medication treatment approach is to reduce the frequency and duration of atrial fibrillation and thereby reducing the severity of symptoms associated with atrial
fibrillation. These medications will not eliminate atrial fibrillation completely, and you will likely continue to have occasional breakthrough episodes.
• These medications are more effective in preventing AF episodes from starting, and much less effective in stopping an episode after it has begun. Therefore, these drugs are best taken on a standing (daily) basis. Once you are in atrial fibrillation, you may need a cardioversion (electrical shock) to get you back to normal rhythm, even when taking one of these medications.
What Antiarrhythmic Medications are available?
There are two main categories of medications that can suppress atrial fibrillation from coming out: sodium channel blockers and potassium channel blockers. Your actual serum sodium and potassium blood levels have nothing to do with these medications.
1. Sodium channel blockers
a. Flecainide (Tambocor), propafenone (Rythmol)
i. Often considered as the first drug of choice in patients with normal heart condition.
ii. These medications can cause dangerous rhythm called ventricular tachycardia in patients with heart disease, so every patient needs to be screened for any heart disease before starting these medications and will need to repeat screening test periodically.
iii. These medications are usually very well tolerated, but at times can cause side-effects such as dizziness, lightheadedness, headache, upset stomach, metallic paste (propafenone), among other side-effects.
2. Potassium channel blockers
a. Sotalol (Betapace), dofetilide (Tikosyn), dronedarone (Multaq), amiodarone (Cordarone)
i. These medications can sometimes slow down your heart rate too much and are usually not used in patients whose heart rate is already slow at baseline (eg, less than 60 beats per minute).
ii. These medications can also rarely cause a dangerous arrhythmia called ventricular tachycardia/Torsades de pointe. This is more likely in patients with very slow heart rates or have underlying structural heart disease. It rarely occurs if you are screened and monitored appropriately. ECG needs to be monitored before and after starting these medications to make sure there is no abnormal change (QT prolongation). For this reason, some of these drugs (eg, dofetilide) require hospitalization for 2-3 days for initiation of the medication so that you can be monitored closely.
iii. Amiodarone is by far the most effective rhythm controlling medication that we have. However, it has several potentially serious side-effects and toxicities, especially when used at a higher dose for extended periods. This medication requires close monitoring with routine blood testing, chest x-ray, eye exam, and close follow up visits. When used properly, this can be an immensely helpful medication for patients with refractory or advanced stages of atrial fibrillation.
What is an ablation?
We don’t know exactly what causes atrial fibrillation. However, we have learned that AF is often initiated by abnormal triggers originating from certain regions of the atria. These triggers tend to be concentrated around the openings of the pulmonary veins in the left upper chamber (left atrium). The pulmonary veins are the blood vessels that drain blood back into the heart after picking up oxygen from the lungs. We have also learned how to eliminate those abnormal triggers either by cauterizing with radiofrequency energy, freezing with cryo energy, or more recently by a short burst of high electrical energy (pulse field). At our center, we use mostly radiofrequency or pulse field energy. Although AF ablation cannot cure atrial fibrillation, through these methods, we can often achieve long term remission for patients with atrial fibrillation for many years without any additional medications.
El Camino Hospital. Atrial Fibrillation Catheter Ablation and Recovery Booklet.
In patients without structural heart disease and who have paroxysmal atrial fibrillation (earliest stage), ablation success rate is 80-90% for remission. Once it reaches the persistent stage, success rates are reduced along with increased need for multiple ablation procedures.
With our experience in the last 20+ years, potential serious or life-threatening complications has been less than 1%. These potential serious complications include stroke, heart attack, blood clots to different parts of the body, narrowing of pulmonary veins, damaging esophagus that runs just behind the heart, diaphragm paralysis, major bleeding in the chest that may require an emergent open-heart surgery to repair, life-threatening rhythm problems, anesthesia related complications, and very rarely, death.
An AF ablation procedure typically involves 1-2 hours of procedural time under general anesthesia. Prior to the ablation, we perform a special ultrasound of the heart, (transesophageal echocardiogram (TEE) to ensure there are no blood clots present that could increase risk of stroke; this technology can identify a blood clot as small as 2mm in size.
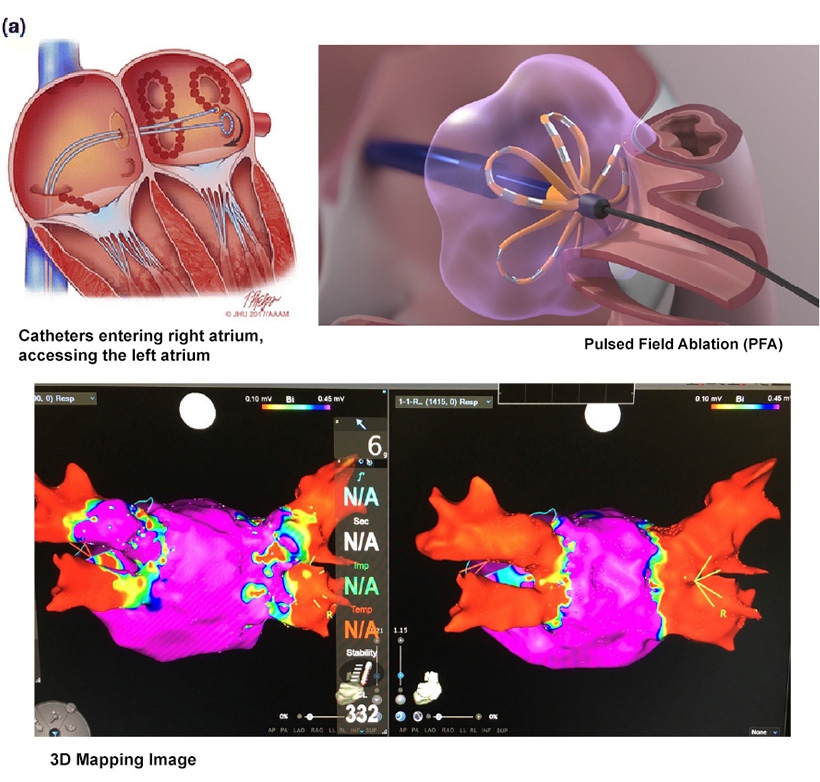
Once we determine that there is no blood clot inside the heart, we place two intravenous sheaths (IV ports with one-way valves) in the femoral vein near the groin. These intravenous sheaths allow us to thread catheters (a thin wire with electrodes at the tip) into the blood stream to the right atrium of the heart. To access the left atrium, a temporary puncture in the wall separating the two atria is performed using a very small needle. This is carefully guided using ultrasound to directly visualize the anatomy. Once in the left atrium, we create a three-dimensional virtual model of the left atrium, and pulmonary veins is created.
Boston Scientific. FARAPULSE, Pulse Field Ablation System. https://www.farapulse.com/us/en/hcp/home.html
The abnormal triggers responsible for atrial fibrillation are identified as abnormal signals called pulmonary vein potentials recorded near the opening of the pulmonary veins. We then target these areas with pulmonary vein potential signals using a catheter with a special tip that can deliver either radiofrequency energy or high electrical energy to eliminate these abnormal circuits. Our end point is to eliminate all the pulmonary vein potentials around all 4 pulmonary veins. In patients with more advanced stages of atrial fibrillation, additional ablations targeting other areas within the left atrium may be required. Throughout the procedure, intravenous blood thinners are administered to minimize the chance of blood clots forming during the procedure. Once the procedure is completed, all the catheters and sheaths are removed. The venous puncture sites are closed with a collagen plug or venous suture device. The patient is awakened and recovered in the post anesthesia unit. The patient must lie flat for 1-3 hours with legs straight after the completion of the procedure to facilitate healing of the puncture site. Patients may then sit up, sit in a chair or walk short distances that evening.
Generally, patients are discharged the same day following observation. Once a patient is discharged from the hospital, he/she can slowly resume usual daily activities, but needs to avoid vigorous activities, e.g. brisk walks, running, exercise, or lifting more than 5 pounds for 7 days to make sure the leg vein puncture site heals properly. Excessive activity or straining too early after the procedure can potentially cause bleeding from the puncture site.
It is important to note that once an ablation is performed, we often do not see the full ablation effect for up to 3 months. In fact, because a patient's heart may be irritated due to inflammation immediately after ablation, it is not unusual to have a period of increased AF for a few weeks after ablation. As the inflammation settles down and ablation sites heal, we start seeing full ablation effect, and eventually elimination of atrial fibrillation.
Please refer to our other brochure on atrial fibrillation ablation for details on how to prepare for the procedure.
What is a cardioversion? Does it treat Atrial Fibrillation?
Cardioversion is a method to reset atrial fibrillation back to normal rhythm. This is performed in the hospital as a same day outpatient procedure. It requires a brief period of deep anesthesia for a few minutes. after adequate anesthesia, an electrical shock is delivered between two electrical pads placed on the chest, front and back. Because of the required anesthesia, the patient cannot drive for the remainder of the day so will require someone to pick them up after the procedure. While it is a very effective way to reset atrial fibrillation back to normal rhythm, it does not affect the likelihood of future atrial fibrillation. Atrial fibrillation can recur at any time after a cardioversion.
Is a pacemaker helpful to treat Atrial Fibrillation?
Pacemakers do not treat directly treat atrial fibrillation. However, in certain situations, a pacemaker implant may be required to allow other treatments for atrial fibrillation (e.g., rate slowing medications or antiarrhythmic medications) when the patient’s baseline heart rate is too slow to allow safe use of these agents. Also, as a last resort, a pacemaker in conjunction with a procedure to electrically uncouple the upper and lower chambers (known as an AV node ablation) may be considered in a patient who has exhausted other treatment options. This approach does not eliminate atrial fibrillation but allows the patient's heart to beat regularly by a pacemaker taking over the rhythm and may reduce symptoms and allow elimination of some medications.
Can I change my lifestyle to improve Atrial Fibrillation?
Several factors have been correlated with the development of atrial fibrillation. These habits and triggers include:
• Alcohol
• Caffeine
• Sleep disturbance
• Dehydration
• Stimulants (e.g., decongestant)
• Sleep apnea
• Major illness
• Major surgery

Although addressing these factors aggressively will not likely fully eliminate the chance of AF recurrence, studies show reducing exposure from these lifestyle habits and triggers may significantly reduce the frequency of atrial fibrillation.

American Heart Association (AHA). The Easy Way to Eat Healthy Infographic. https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/nutrition-basics/what-is-a-healthy-diet-recommended-serving-infographic
How do I know what treatment is best for my atrial fibrillation? What things should I consider in deciding what treatment I should choose?
There are several important factors to consider in choosing which treatment option is most appropriate for your atrial fibrillation. First and foremost, should be determining how much AF is affecting your daily activities and quality of life. Alleviation of symptoms is the primary benefit of treatments such as antiarrhythmic medications or AF ablation. However, due to the potential damage AF may cause to heart function and the stroke risk associated with AF, there may be benefits from treatment beyond symptom relief. Increasingly, studies are showing potential survival benefit even in those patients with mild symptoms.