
Accessibility Project: “Evaluating the Effect of Team-based Care Model on Workflow Efficiency, Patient Satisfaction, and Cost-Effectiveness in One Cardiology Department”
In the U.S., the average waiting time to see a cardiologist is 38 days, with longer times for non-urgent cases. Contributing factors include:
- Staff shortages
- Clinician burnout
- Inefficient clinical workflows
The Palo Alto Medical Foundation (PAMF) Cardiology department piloted a team-based care model.
- A nurse and medical assistant were trained to facilitate patients’ pre-visit preparation, care system navigation, on-site education, and follow-up visits.
_____________________________________________________________________________________________________________________________________________________________
Traditional Model vs. Team-based Care Model
|
Traditional Model |
Team-based Care Model |
 |
 |
Challenges in Current Workflow
-
Physician-centered model
- Physicians handle all aspects of the new patient visits, including ordering tests, prescriptions, and documentation in EPIC
- Pre-visit chart review and records gathering take 15-30 minutes per patient
-
Limited Access and Inefficient Scheduling
- Routine new patient visits book 8-12 weeks out
- Manual triage by physicians due to inappropriate referrals and lack of referral intake coordinator
- Time-consuming back-and-forth between staff for urgent cases
- Scheduling based on next availability rather than patient needs
- Urgency flags often overlooked
-
Staffing Constraints
- High nurse dependency (coverage gaps burden MDs)
- MA turnover and limited clinical judgement impact patient prep
- No defined navigator to manage logistics or follow-up
- MD reports 40% of work as frustrating (ideal would be only 15% frustrating or less)
-
Workflow Inefficiencies
- Patients arrive unprepared without needed diagnostics tests, leading to repeat visits and delays
- Providers spend significant time on chart prep
-
Gaps in Patient Education
- No standardized materials, described as “hit or miss”
- Heavy reliance on verbal explanations (repetitive)
- Lacks multimedia tools — no videos, FAQs, or visuals
Team-Based Care Model
Primary Objectives
- Evaluate the impact of the new care model on patient’s accessibility to cardiologist and patient/clinician’s experience
- Cost Effectiveness
- Implementation experience
Primary Outcomes
- Time to see a cardiologist
- Time allocation related to a visit
- Patient experience
- Cardiologist experience
- Clinical Team experience
Study Period: 12-month before implementation of a new care model, and 6-month after the implementation.
NEW WORKFLOW SUMMARY
| PRE-VISIT | DURING VISIT | POST VISIT |
|
|
|
|
|
- RN summarizes relevant medical records and coordinates diagnostic testing before appointments
- Physician pre-visit prep now takes only 5-10 minutes
- RN handles all post-consult documentation and patient education, reducing physician’s administrative load
- Navigator schedules follow-up tests and appointments, and communicates with patients via MHO
Benefits of New Model
- Reduced New Patient Wait Time: From 6-8 weeks to under 2 weeks
- Improved Physician Satisfaction: Physician spends nearly all face-to-face time on clinical care rather than documentation; shifted from 75/25 positive/negative to over 90% positive
- More Efficient Visits: Physicians have complete data during the consult, enabling better decision-making
- Improved Patient Experience: Patients arrive with all needed tests results, avoiding needing multiple visits for tests and follow-up; patients have direct RN and navigator contact
- Better RN Utilization: RN provides extended education and follow-up, which patients report appreciating
- Reduces Physician and Nurse Burden: Frees up time for physicians and triage nurses
Patient-Reported Experience
Case and Control groups reported similar levels of overall satisfaction, though not statistically significant, case patients reported having less anxiety than control patients (65.31% vs. 76.32%).
|
Question |
Control |
Case |
P-value |
|
Timely scheduling with cardiologist |
48.68% |
72.28% |
0.001 |
|
Were you instructed to complete any pre-visit tests? |
18.92% |
53.06% |
>0.001 |
|
How satisfied were you with any pre-visit communication? |
54.17% |
68.75% |
0.098 |
|
Recommend this facility to family and friends |
67.11% |
78.35% |
0.097 |
Overview of Study Outcome
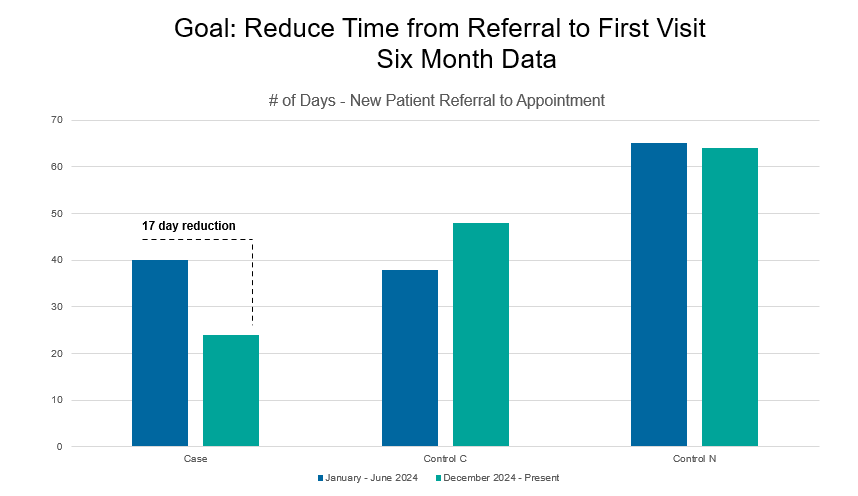
- The new care model significantly reduced patient wait times to see a cardiologist, from 41 days to 24 days (41% reduction), an absolute decrease of 30 days.
- Cardiologist time with patients decreased to 15 minutes; however, patients spent an additional 11 minutes with the NP for education and post-visit coordination.
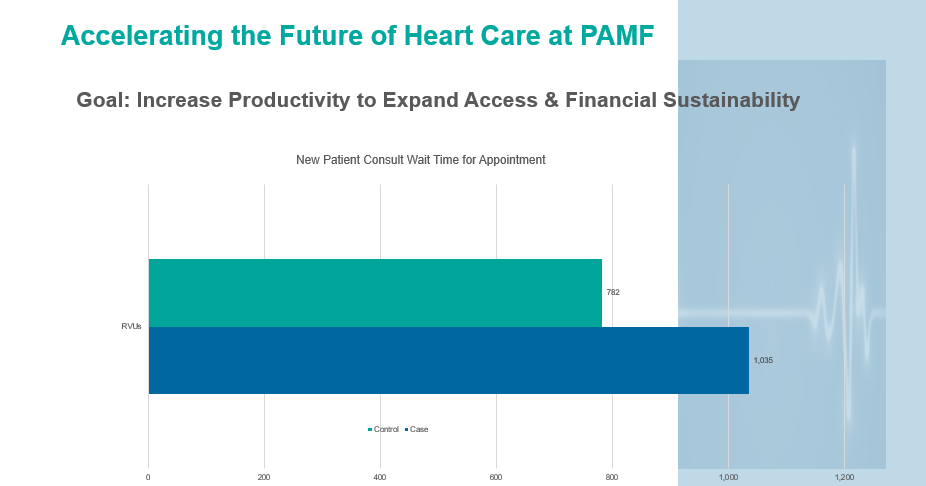
- Total RVUs for new consult patients increased significantly at the department level.
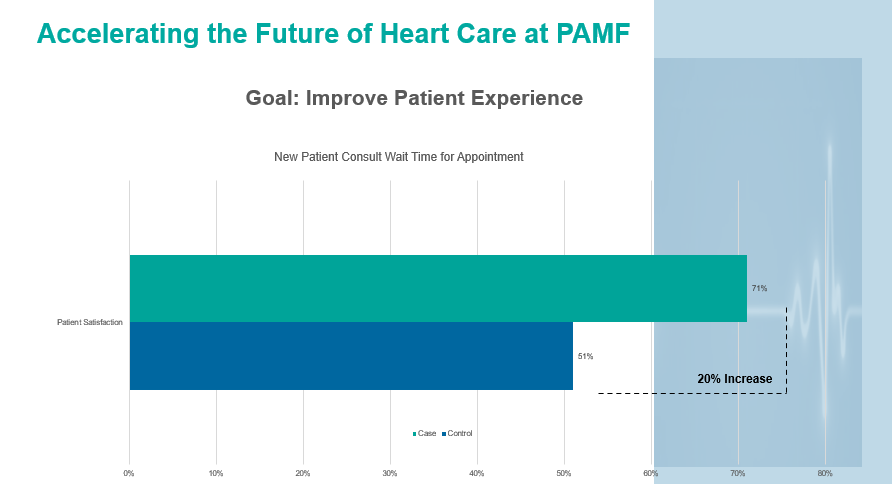
- The new care model improved patient satisfaction with scheduling, visit preparation, and overall workflow.
- Cardiologists reported reduced burnout.
Ongoing Challenges & Areas of Additional Improvements
|
Challenges |
Areas for Improvements |
| Manual retrieval of records (e.g., faxes, EKGs) is time-consuming | Delegate record retrieval tasks for a support staff member |
| Scheduling tests across departments may disrupt established workflows | Add medical assistant support for scheduling and logistics |
| Lack of standardized patient education materials | Develop and standardize patient education materials |
| Documentation remains a burden, explore tools like Abridge to streamline notetaking | Determine when a patient transitions from “new” to “established” to potentially streamline care |
| Assess optimal physician-to-RN ratio (current estimate = 3-4 physicians per RN) |
ACC Conference Abstract 2026
Evaluating the Effect of a pilot Patient-centered, Team-based Care in Cardiology Department on Workflow Efficiency, Patient Satisfaction, and Cost-effectiveness
Background: On average, the waiting time to see a cardiologist in the US is 38 days, with longer times for non-urgent cases. A cardiology department in northern California piloted a team-based care model for new patient consultations. A nurse was trained to coordinate care, collect labs before and after visits, and provide education, allowing cardiologists to focus on treatment decisions. This study evaluated the model’s efficiency and patient satisfaction.
Methods: The pilot team-based care model was implemented by one cardiologist (case) at a cardiology department in January 2025, with two cardiologists in the same clinic serving as controls (traditional cardiologist-centered model). Time-motion data were collected to evaluate the time spent with clinical staff during a visit. Patient satisfaction was assessed by survey, and staff feedback collected by interviews. Electronic Health Record (EHR) data on referrals, appointments, and relative value units (RVUs) were extracted for the pre-intervention (2024) and intervention periods (2025). Patient waiting time, satisfaction, and RVU were compared between case and control.
Results: In the first quarter of 2024 (Q1 2024), the average referral-to-appointment time was 41 days (std=55.75) for case and 48 days (std=39.26) for controls (not significant). During the first quarter of 2025 (Q1 2025), 84 new patients were seen by the case and 76 by controls. Wait time decreased to 24 days (std=17.40) for the case but remained 44 days (std=30.91) for controls. Among patients, 71% reported being “very satisfied” in timely scheduling of visits with the case cardiologist, which was significantly higher than for controls (51%). In addition, 53% of the team-based model reported satisfaction with pre-visit preparation versus 21% for controls. Cumulative RVU from 30 days pre- and post-initial encounter were 623 for case and 806 for controls in Q1 2024. By Q1 2025, RVUs increased to 1035 for the case and decreased to 782 for controls, an absolute increase of 436 RVUs for the team-based model.
Conclusion: The piloted team-based model substantially reduced patient wait times, improved satisfaction, and increased RVU generation.
AF Outcome Project: “Using Large Language Model to Automatically Capture Patient Risk and Outcomes after Atrial Fibrillation Ablation”
Atrial Fibrillation (AF) is the most common arrhythmia. The incidence and prevalence of Atrial Fibrillation (AF) increased 3-fold over the last 50 years. Numerous randomized controlled trials have shown that catheter ablation, an advanced treatment to restore normal heart rhythm for AF patients) demonstrates superior results for restoration of normal sinus rhythm. However, study on the success and adverse effect of AF ablation procedure in the real-world setting is lacking due to one main challenge-clinical symptoms usually appear within 1 week and vary from individual to individual after an ablation procedure, and those symptoms are mostly documented in the encounter notes in subsequent clinical visits. It is extremely challenging and time-consuming to speculate and flag the success rate and potential adverse effects for this procedure, furthermore, the adverse event, if not observed or address timely, it imposes significantly negative impact on the patient outcome, including death. If not conducted systematically and in standardized manner, the adverse effect was easy to miss since it requires manual reviewing progress notes from the procedure, follow-up visit, and in combination with lab results and related complications (i.e., diagnosis) in the subsequent encounters.
Therefore, we propose to pilot test a strategy of using LLMs to report success and further extract adverse effects for patients who went through AF ablation procedures and validate LLM output with the chart-review result, a gold-standard. If successful, it can be implemented in electrophysiology departments to capture and alert clinicians to manage adverse effects.
It is a retrospective cohort study based on comprehensive electronic health records (EHR) data from 2015-8/31/2025, including structured data and free text data. Patients who have gone through Atrial Fibrillation ablation procedures at Sutter cardiology departments are included in the analysis.