
Atrial Flutter (AFL) is a type of heart rhythm disorder (arrhythmia) caused by an electrical “short circuit” in the upper chambers of your heart (the atria). This causes the atria to beat very fast—usually around 240 to 300 times per minute—which can prevent the heart from pumping blood efficiently.
Typical vs. Atypical Atrial Flutter
While both involve a “loop” of electrical activity, the location of that loop determines the type.
Typical Atrial Flutter
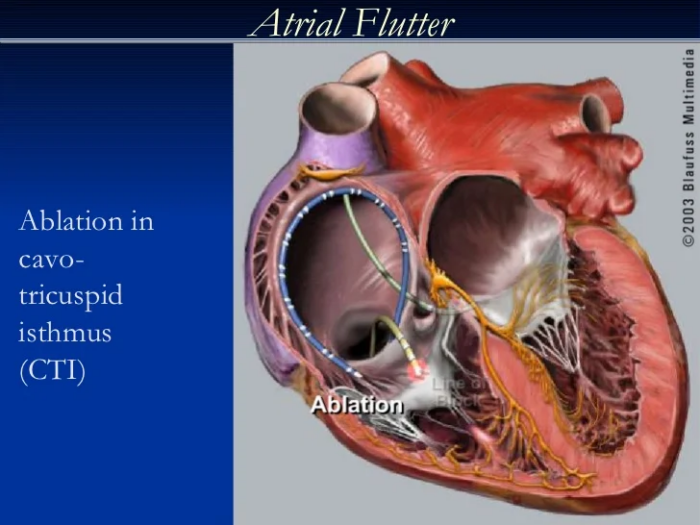
This is the most common type of atrial flutter. Its circuit is well-defined and forms a predictable reentrant pathway around the tricuspid valve in the right atrium. This type is generally very responsive to catheter ablation. This high responsiveness to catheter ablation makes it an ideal target for treatment, often resulting in successful long-term management of atrial flutter.
Typical atrial flutter ECG shows a hallmark sign of “sawtooth pattern” that represents “flutter waves”.
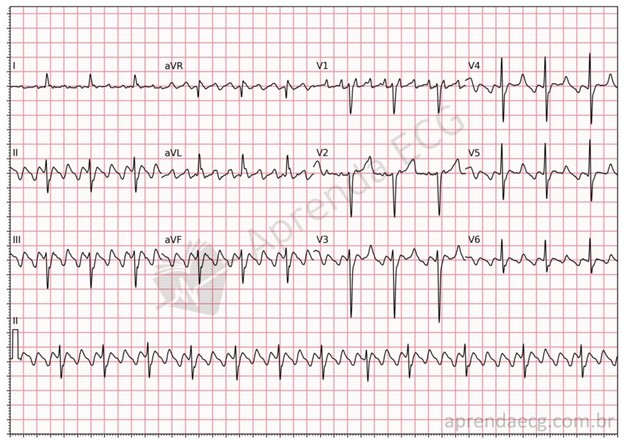
Typical atrial flutter will eventually progress into atrial fibrillation if left untreated. Even in patients who undergo a successful catheter ablation for typical atrial flutter, there is at least 20-25% chance that they will eventually develop atrial fibrillation in the future. Patients should work closely with their healthcare providers to regularly monitor for signs of atrial fibrillation through scheduled check-ups and appropriate diagnostic tests.
Atypical Atrial Flutter
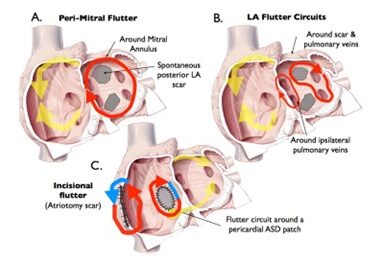
Unlike the well-defined and predictable reentrant circuit seen in typical atrial flutter, the circuit in atypical atrial flutter can occur in various locations within either the right or left atrium. This variability in circuit location means that mapping and targeting the abnormal electrical pathway during catheter ablation is more challenging, and at times reduces success rate. Atypical atrial flutter can be associated with previous heart surgery surgery/procedures, or other heart conditions resulting in atrial scars.
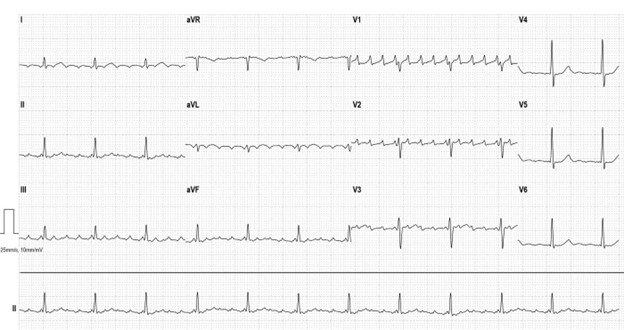
Unlike typical atrial flutter ECG which usually has same appearance, atypical atrial flutter ECG can vary depending on the location of its circuit.
American Journal of Cardiology. Treadmill Stress Test in a 56-year-old Man. https://www.ajconline.org/article/S0002-9149(19)30939-7/abstract
Atypical atrial flutter frequently leads to, or coexists with, atrial fibrillation. Therefore, atrial fibrillation ablation is often done along with atypical atrial flutter ablation at the same time.
Common Symptoms
In both typical and atypical atrial flutter, patients may feel no symptoms at all, while others may experience:
- Palpitations: A sensation of a racing, fluttering, or “flopping” heartbeat.
- Shortness of Breath: Especially during physical activity.
- Fatigue: Feeling unusually tired or weak.
- Lightheadedness: Feeling dizzy or faint.
- Chest Pain: Mild discomfort or pressure.
The Risk of Stroke
When the heart flutters, both in typical and atypical atrial flutter, blood can pool in the atria rather than moving smoothly into the lower chambers. This pooling can lead to blood clots.
*Important: If a clot forms and travels to the brain, it causes a stroke. Without proper anticoagulation (blood thinners), the risk of stroke is significantly higher, even if you don’t feel “sick.”
Treatment Options
-
Anticoagulation (Blood Thinners)
- For patients at moderate to high risk for stroke, blood thinning medications (anticoagulants) are usually recommended unless there is a significant contraindication such as major bleeding risk or high risk of falls. Unlike older blood thinners (e.g. warfarin/Coumadin), newer anticoagulants known as DOACs, (direct oral anticoagulants) such as apixaban (Eliquis) and rivaroxaban (Xarelto) are much easier to use. They have fewer interactions with other medications, and do not require dietary restrictions or frequent blood tests. They are safer because they are absorbed and broken down by the body in a very predicable way. These medications have been shown in large clinical trials to significantly reduce the risk of stroke. Because these are potent blood thinners, it is important to avoid activities that increase the risk of injury or falls. Activities such as riding bicycles or motorcycles, engaging in contact sports, downhill skiing, climbing ladders, or using power tools should be avoided. For some patients, using a walking stick, cane, or walker may help improve balance and reduce the risk of falls. You should also avoid other blood thinning medications such as aspirin, ibuprofen, or other non-steroidal anti-inflammatory medications unless specifically approved by your physician.
- It is advisable to wear a medical ID bracelet or necklace to identify that you are taking a blood thinning medication. Most emergency departments carry a reversing agent for blood thinners, and it is particularly important for emergency personnel to know that you are on a blood thinning medication in case of serious injury or bleeding. 

-
Antiarrhythmic Agents
- There are two important things you need to know about a rhythm controlling medication (Antiarrhythmic medication) approach:
- The goal of a medication treatment approach is to reduce the frequency and duration of typical/atypical atrial flutter and thereby reducing the severity of symptoms associated with it. These medications will not eliminate atrial flutter completely, and you will likely continue to have occasional breakthrough episodes.
- These medications are more effective in preventing atrial flutter episodes from starting, and much less effective in stopping an episode after it has begun. Therefore, these drugs are best taken on a standing (daily) basis. Once you are in atrial flutter, you may need a cardioversion (electrical shock) to get you back to normal rhythm, even when taking one of these medications.
- Beta-Blockers
- Metoprolol succinate (Toprol), metoprolol tartrate (Lopressor), atenolol (Tenormin)
- Beta-blockers slow your heart rate and lower your blood pressure (often used as blood pressure controlling agent).
- Potential side-effects can be fatigue, shortness of breath (especially if you have history of lung problems such as asthma or COPD (Chronic Obstructive Pulmonary Disease), dizziness/lightheadedness, especially if it slows down your heart rate or lowers your blood pressure too much. At higher doses, some may experience weight gain, erectile dysfunction, and depression.
- Calcium Channel Blockers
- Diltiazem (Cardizem), Verapamil (Calan)
- Calcium channel blockers also lower your blood pressure (often used as blood pressure controlling agent).
- Potential side-effects include ankle/feet swelling, constipation, dizziness/lightheadedness, especially if your blood pressure gets too low.
- Digoxin
- This is an old drug that is rarely used as a primary agent to slow down heart rate.
- It is mostly used when a patient’s blood pressure is too low to use beta blockers or calcium channel blockers since, unlike those drugs, digoxin does not have an effect on blood pressure.
- This medication requires close blood level monitoring (blood tests).
- There are two important things you need to know about a rhythm controlling medication (Antiarrhythmic medication) approach:
-
Catheter Ablation
- Typical Atrial Flutter Ablation: The procedure has a 90% success rate in eliminating the typical atrial flutter circuit, with serious complications occurring in less than 1% of cases.A cardiac electrophysiologist inserts a catheter through a leg vein into the right atrium, then uses radiofrequency energy to cauterize the area involved in typical atrial flutter. The procedure is usually done under general anesthesia on an outpatient basis, with short recovery; patients can sit and walk the same evening but should avoid heavy lifting or strenuous activity for a week. 
- Atypical Atrial Flutter Ablation: Eliminating atypical atrial flutter can be difficult due to its variable location in the atria and potential involvement of multiple circuits. Success rates drop further if the patient is not actively experiencing atypical atrial flutter during ablation, as the circuit is harder to identify. Overall, success rates range from 70–90%. A cardiac electrophysiologist inserts a catheter through a leg vein into the right and/or left atrium, then uses radiofrequency or pulsed field energy to eliminate the area involved in atypical atrial flutter. The procedure is usually done under general anesthesia on an outpatient basis, with short recovery; patients can sit and walk the same evening but should avoid heavy lifting or strenuous activity for a week. 
- Typical Atrial Flutter Ablation: The procedure has a 90% success rate in eliminating the typical atrial flutter circuit, with serious complications occurring in less than 1% of cases.A cardiac electrophysiologist inserts a catheter through a leg vein into the right atrium, then uses radiofrequency energy to cauterize the area involved in typical atrial flutter. The procedure is usually done under general anesthesia on an outpatient basis, with short recovery; patients can sit and walk the same evening but should avoid heavy lifting or strenuous activity for a week. 
One Heart Cardiology. https://oneheartcardiology.com.au/carousel_slide/abnormal-heart-rhythm-3/