
What are Premature Atrial Complexes (PACs)?
Imagine your heart is a drummer, keeping a steady, regular beat.
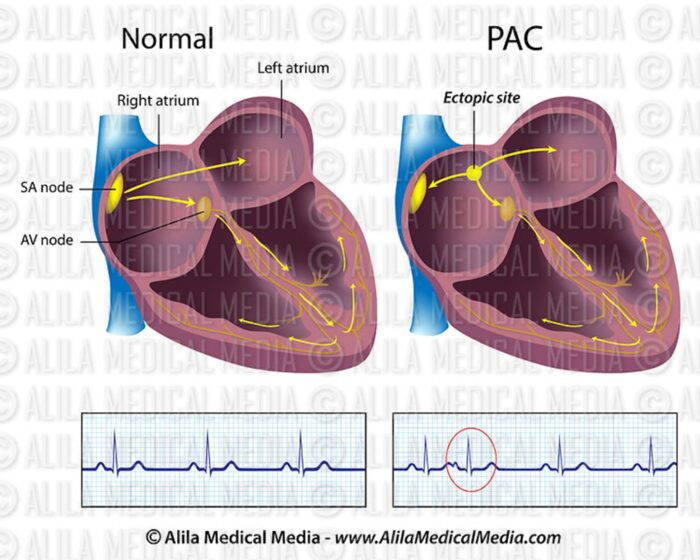
- Your heart has four chambers: two upper chambers called the atria, and two lower chambers called the ventricles.
- A special spot in the upper right chamber called SA node (the natural pacemaker) sends a regular electrical signal to make your heartbeat.
- A Premature Atrial Complex (PAC) is when an extra electrical signal starts too early in the upper chambers (can be from left or right atria). This extra signal causes the heart to beat too soon.
What does it feel like?
Most of the time, PACs are harmless and cause no symptoms. However, if you do feel them, people often describe a sensation like:
- A “skipped” or “missed” beat.
- A flutter or palpitation in the chest.
- A strong, pounding beat after the early one (this is often the next normal beat trying to catch up).
PACs are common and are often not a sign of serious heart disease. They can happen to anyone, even healthy people.
What tests are needed to diagnose PACs?
- ECG: This is typically performed in a doctor’s office, urgent care, emergency department, or hospital setting.
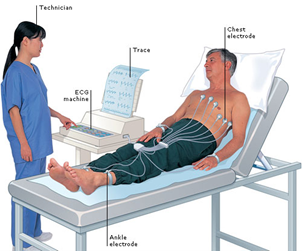 Small electrodes (stickers) are placed on your chest, arms, and legs, then a 12-lead ECG/EKG is recorded.
Small electrodes (stickers) are placed on your chest, arms, and legs, then a 12-lead ECG/EKG is recorded.
- Ambulatory Monitor: A small patch about the size of your palm is placed on your chest for 2-4 weeks to record rhythm continuously. You can take a shower
 and carry on most activities while wearing this monitor, although swimming should be avoided.
and carry on most activities while wearing this monitor, although swimming should be avoided.
- Wearable Devices: Apple Watch/Kardia/FitBit/Android smartwatch/other wearable monitors may not be effective in documenting PACs
 because it is too brief for you to be able to capture it by trying to record it when it occurs although if you are having frequent episodes, you may be able to capture it during a typical 30 second wearable monitor recording period.
because it is too brief for you to be able to capture it by trying to record it when it occurs although if you are having frequent episodes, you may be able to capture it during a typical 30 second wearable monitor recording period.
Are PACs dangerous?
PACs are considered benign. They do not increase risk of stroke and certainly do not cause heart attack. However, they can cause symptoms that can affect your quality of life, and in rare instances, they can increase risk of atrial fibrillation if you have high number of PACs.
When should PACs be treated?
Treatment often depends on whether you have symptoms, how often the PACs occur, and if they are linked to other heart conditions. For many people, PACs do not need treatment at all.
You can consider a treatment for PACs in below situations:
- Symptoms from PACs are affecting your quality of life, e.g. preventing you from doing things you like to do.
- Very high frequency of your PACs that could potentially increase chance of developing a rhythm atrial fibrillation
- If lifestyle changes don’t work, or if your symptoms are frequent and disruptive, your doctor may prescribe medication.
How are PACs treated?
Lifestyle Changes (Often the First Step)
Because PACs can often be triggered by outside factors, the simplest and safest treatment is to make changes to your daily habits:
- Reduce Stimulants: Things like caffeine (in coffee, tea, soda, energy drinks) and alcohol can make your heart more sensitive and trigger PACs. Cutting back on or eliminating these can often significantly reduce the frequency of PACs. Decongestants is also a stimulant and can be a trigger for PACs.
- Managing Stress and Anxiety: High stress and strong emotions are common triggers for heart palpitations. Techniques like deep breathing, meditation, or light exercise may help.
- Quit Smoking: Nicotine is a major stimulant that irritates the heart.
- Stay Hydrated: Dehydration can sometimes be a trigger.
Medications (Anti-Arrhythmic Drugs)
- Beta-Blockers and Calcium Channel Blockers: These are often the first medications doctors try. They work by slowing the heartrate and making the heart muscle less exciting, which helps to regulate the rhythm. They are often used to treating high blood pressure as well.
- Other Anti-Arrhythmic Medications (e.g., Flecanide, Sotalol, Amiodarone): If the first-line medications are not effective, your doctor may recommend stronger drugs. These medications specifically work on the electrical system of the heart to prevent extra, early beats.
- **Important Note: These medications can have serious side effects and are usually reserved for frequent or highly symptomatic PACs. Your doctor will carefully weigh the benefits against the risks.
Beta-Blockers
- Metoprolol succinate (Toprol), Metoprolol tartrate (Lopressor), Atenolol (Tenormin)
- Beta-blockers slow your heartrate and lower your blood pressure (often used as blood pressure controlling agent).
- Potential side-effects can be fatigue, shortness of breath (especially if you have history of lung problems such as asthma or COPD (Chronic Obstructive Pulmonary Disease)), dizziness or lightheadedness, it may slow down your heartrate or lower your blood pressure too much. At higher doses, some may experience weight gain, erectile dysfunction, and depression.
Calcium Channel Blockers
- Diltiazem (Cardizem), Verapamil (Calan)
- Calcium channel blockers also lower your blood pressure (often used as blood pressure controlling agent)
- Potential side-effects include ankle/feet swelling, constipation, dizziness/lightheadedness, especially if your blood pressure gets too low.
Sodium Channel Blockers
- Flecanide (Tambacor), Propafenone (Rythmol)
- These medications can cause dangerous rhythm called ventricular tachycardia in patients with heart disease, so every patient needs to be screened for any heart disease before starting these medications and will need to repeat screening test periodically.
- These medications are usually very well tolerated, but at times can cause side effects such as dizziness, lightheadedness, headache, upset stomach, metallic taste (propafenone), among other side-effects.
Potassium Channel Blockers
- Sotalol (Betapace), Dofetilide (Tikosyn), Dronedarone (Multaq), Amiodarone (Cordarone)
- These medications can sometimes slow down your heartrate too much and are usually not used in patients whose heartrate is already slow at baseline (e.g., less than 60 beats per minute).
- These medications can also rarely cause a dangerous arrhythmia called ventricular tachycardia/Torsade’s de pointe. This is more likely in patients with very slowly heartrates or have underlying structural heart disease. It rarely occurs if you are screened and monitored appropriately. ECG needs to be monitored before and after starting these medications to make sure there is no abnormal change (QT prolongation). For this reason, some of these drugs (e.g.dofetilide) require hospitalization for 2-3 days for initiation of the medication so that you can be monitored closely.
- Amiodarone is by far the most effective rhythm controlling medication that we have. However, it has several potentially serious side-effects and toxicities, especially when used at a higher dose for extended periods. This medication requires close monitoring routine blood testing, chest x-ray, eye exam, and close follow-up visits. When used properly, this can be an immensely helpful medication for patients with refractory or advanced stages of atrial fibrillation. Amiodarone can cause sensitivity to sun. When taking amiodarone, you should use strong sunscreen and consider wearing a hat and long sleeves when possible.
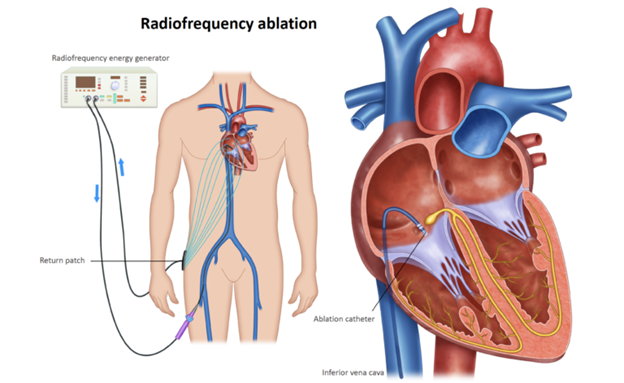
Catheter Ablation (Procedure)
In rare situations, if PACs are very frequent, cause severe symptoms, and do not respond well to medications or lifestyle changes, your doctor may recommend a procedure called catheter ablation.
What it is: This is a minimally invasive procedure done by a heart rhythm specialist (electrophysiologist).
How it works:
- A long, flexible tube (catheter) is threaded through a blood vessel (usually in the groin) up to the heart.
- The doctor uses special tools to map the electrical signals and pinpoint the exact small area of heart tissue that is firing the extra, premature signals.
- A burst of energy (usually heat or cold) is delivered through the catheter to safely destroy (ablate) this tiny piece of problem tissue.
- The scar tissue that forms stop the abnormal electrical signal from starting, which eliminates the PACs.
Journal of Cardiothoracic and Vascular Anesthesia. Mechanical Circulatory Support for Acute Myocardial Infarction Cardiogenic Shock: Review and Recent Updates. https://www.jcvaonline.com/article/S1053-0770(24)00945-5/abstract
Download our Your Guide to Premature Atrial Complexes (PACs) PDF.